AUCTORES
Globalize your Research

Review Article | DOI: https://doi.org/10.31579/2640-1053/066
1 Servei d’Immunologia, Hospital Clínic de Barcelona, University of Barcelona, Institut d'Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS). Barcelona, Spain.
1,2 Platform d’Immunoteràpia Hospital Sant Joan de Déu- Clínic. Platform d’Immunoteràpia Banc de Sang I Teixits-Clínic. Barcelona, Spain.
3 Functional Unit of Clinical Immunology, Sant Joan de Déu-Hospital Clinic, Barcelona, Spain.
*Corresponding Author: Manel Juan, Servei d’Immunologia, Hospital Clínic de Barcelona, University of Barcelona, Institut d'Investigacions Biomèdiques August. Barcelona, Spain
Citation: Muñoz-Sánchez G , Betriu S, Esteve-Solé A.3, Ortiz de Landázuri I, González-Navarro E.A, Español-Rego M, San Bartolomé C, Egri N, Palou E, Juan M. Tregs and Other Suppressive/Regulatory/Tolerogenic Cell Therapies in Transplantation, J. Cancer Research and Cellular Therapeutics. Doi: 10.31579/2640-1053/066
Copyright: © 2020 Manel Juan, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium,provided the original author and source are credited.
Received: 30 December 2019 | Accepted: 06 January 2020 | Published: 07 January 2020
Keywords: treg; transplantation; rejection; cell therapy
Poor long-term graft outcome remains problematic because of the inability to prevent chronic allograft rejection. Strategies based on suppression/regulation/tolerance (3 different but similarly used concepts) of the immune system often leads to other concerns. New alternatives based on facilitating the induction of alloantigen tolerance by regulatory T cells (Tregs) and other immune-suppressor cells can restore the balance between inhibitory and effector arm. This review mainly summarizes results about the use of Tregs for the control of transplant rejection, commenting also other situations and potentially similar cell therapies.
Poor long-term graft outcome remains problematic because of the inability to prevent chronic allograft rejection. Strategies based on suppression/regulation/tolerance (3 different but similarly used concepts) of the immune system often leads to other concerns. New alternatives based on facilitating the induction of alloantigen tolerance by regulatory T cells (Tregs) and other immune-suppressor cells can restore the balance between inhibitory and effector arm. This review mainly summarizes results about the use of Tregs for the control of transplant rejection, commenting also other situations and potentially similar cell therapies.
Organ transplantation is currently a successful treatment for the majority of patients with end-stage organ failure. Fortunately, improvement in transplant technology, non-invasive biomarkers, better selection of donors and recipients by Human Leukocyte Antigen (HLA) typing/compatibility and the advance of immunosuppresive agents have enabled clear progress in transplantation outcomes ameliorating the graft survival, at least in the early post-transplant stage. However, the poor long-term graft outcome remains problematic because of the inability to prevent chronic allograft rejection (CR). In fact, half of all transplanted kidneys still fail within 15 years after transplantation[1]. In this context, the current treatment of transplantation focuses on the limitation of the effector arm of immune response with nonspecific immunosuppressive drugs (ISD) that perform by inhibiting non-specific T and B cell activation pathways or by depleting lymphocytes.
The mentioned strategy based on suppression of the immune system often leads to over immunosuppression. The lack of specificity of ISD frequently diminishes patient’s quality of life and gives rise to life-threatening infection episodes, malignancies, cardiovascular diseases or kidney failure causing graft loss or even death [2]. Due to the inconveniences caused in transplanted patients by this therapeutic approach, new alternatives that allow better results are being sought. In general, suppression, regulation or tolerance induction are different terms that often are interchangeably used. Although “Suppressor” cells suggest the blockage of responses, “Regulatory” should be a more flexible concept (increase or decrease functions) but just used under the meaning of suppression, and “Tolerogenic” cells are those cells that could induce specific recognition which would program no-response, the three concepts are often used as synonymous. Facilitating the induction of alloantigen tolerance by regulatory T cells (Tregs) and other immune-suppressor cells, restoring the balance between the inhibitory and the effector arm is the aim of a lot of novel strategies based on suppressive/regulatory/tolerogenic cells. Although this review mainly summarizes results about the use of Tregs as controllers of rejection in transplantation, other situations and potential similar cell therapies are also commented.
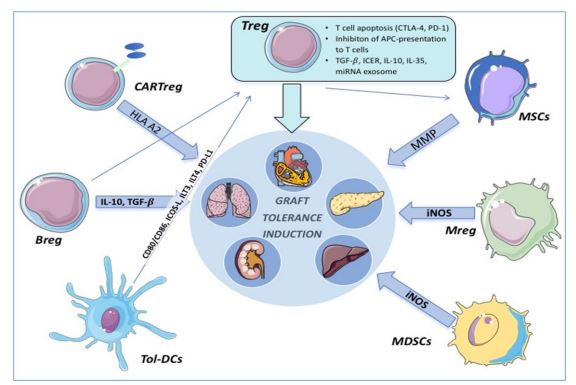
Tregs: Regulatory T-cells; MSCs: Mesenchymal stromal cells; MMP: matrix metalloproteinase; Mregs: regulatory macrophages; MDSCs myeloid-derived suppressor cells; iNOs: inducible NO synthase; Tol-DCs: Tolerogenic DCs; Bregs: Regulatory B cells; CAR-Tregs: Treg cells expressing chimeric antigen receptor. Tregs induce apoptosis of alloreactive T cells via CTLA-4 and PD-1 engagement.
Besides, Tregs prevent APC’s ability to activate effector T cells by CTLA-4 and LAG-3 binding. Other mechanisms such as TGF-β expression, inducible cAMP early repressor (ICER), IL-10 and miRNA exosome transference are also involved. MSCs secrete MMP types 2 and 9 facilitating the cleavage of CD25 expressed on CD4+ T cells. Both Mregs and MDSCs have immunossupressive activity in an iNOS-dependent pathway. Tol-DCs are able to induce Treg development via CD80/86, ICOS-L, ILT3, ILT4 and PD-L1 binding. Bregs can modulate immune homeostasis in an IL-10 dependent pathway or by IL-10-independent mechanisms based on IL-35 or TGF-β

. CAR-Tregs recognize specific antigens such as HLA-A2 supressing allograft rejection.
1. - General concepts about Tregs
1.1. Characterization and Ontogeny
Tregs are a subset of CD4+ T cells (comprising 1-9% of blood CD4+ T cells) whose function is to limit immune responses by maintaining self-tolerance. Tregs are traditionally classified as natural Tregs (thymus-derived), or peripheral inducible Tregs (iTregs), which are the result of natural T-cells when exposed to cytokines such as TGF-β and IL-2p[3,4]. Tregs are distinguished by the high expression of both CD4+ and CD25+ (IL-2 alpha chain Receptor) and by the transcriptional regulator Forkhead Box P3 (FOXP3)[5], which is a reliable marker specially in mouse Tregs. However, FOXP3 is also expressed in human effector T cells when activated[6] and it is required the use of other markers such as CD4+/CD25+/CD127- to characterize them. Additionally, transcription factor FOXP3 demethylation serves to preserve Treg phenotype and related epigenetic changes are now used to identify Tregs in clinical research [7].
Thymic ontogeny of Tregs starts in CD4 single-positive stage (CD4+/CD8-). Upregulation of FOXP3 and consequent differentiation of Tregs depends on a great heterogeneity of paths and cytokines ruled by environmental conditions and is strongly influenced by inflammatory cues. Antigen Presenting Cells (APCs) in thymus promote FOXP3 upregulation in these thymocytes by self-antigen-presenting in the context of self-MHC class II8. This event together with a satisfactory interaction with CD28 in terms of strength, duration and affinity[9] activates nuclear factor-κB (NF-κB), forkhead box protein O (FOXO) and nuclear factor of activated T cells (NFAT)[10], which is required for FOXP3 expression.
Other factors, like the presence of high concentrations of TGF-β[11], Inducible Costimulator (ICOS/ICOSL) and thymic stromal lymphopoietin are also involved[12]. Also, FOXP3 upregulation event promotes Interleukin-2 receptor alpha chain (also called CD25) surface expression allowing cytokine signalling and consequently the development of fully functional Tregs [13].
1.2. Immunosuppressive drugs and Tregs
PI3K-mTOR (mammalian target of rapamycin) signalling pathway is recognized as one of the main targets of ISD used in transplantation. mTOR is a critical signalling molecule with a crucial role in transcribing immunological cues into a specific family of T cells. Extensive studies at the molecular level of this pathway are imperative for unravelling Tregs association with immunosuppresive drugs, cancer and autoimmunity.
How mTOR regulates Treg phenotype and metabolism is not fully understood. mTOR is formed by two complexes named mTOR1(Raptor), the principal target of rapamycin (RAPA), and mTOR2 (Rictor). T cells lacking whole mTOR complex differentiate preferentially into FOXP3+ Treg rather than Th1, Th2 or Th17 effector cells [14] and expand more efficiently in the presence of IL-2 compared with normal-mTOR T cells. It has been suggested that TGF-β mediated induction of Foxp3+ regulatory cells in deficient mTOR T-cells could explain this divergence given that Tregs development is regulated by a protein named Smad3, which is more likely to be stimulated by TGF-β in mTOR-deficient Treg cells. However, mice containing Treg specific deletion of Raptor (mTOR1) lose their Treg function in vivo [15] and develop fatal autoimmune inflammatory state [16].
Many immunosuppressive drugs currently used base their mechanism on the mTOR pathway determining Tregs function and transplantation outcome. For instance, calcineurin inhibitors have shown a negative effect on Tregs generation and function [17] while there is substantial evidence that rapamycin favours Treg survival and function [18]. The effects of mycophenolic acid are variable [19,20] and regarding basiliximab, due to its anti-CD25 effect, may have a deleterious effect on Treg cells [21]. Nonetheless, either via mTOR or by another alternative mechanism there is a widespread observation that the percentage of circulating CD25+ CD4+ FOXP3 cells decreases after transplantation [22]. This way, the balance between immunoreactive and immunosuppressive status gets compromised concluding in the adverse events or reactions described above. That is the main reason why new approaches focusing on tolerance induction via Tregs or other promising methods such as regulatory macrophages or mixed chimerism should be considered.
2. - Tregs in transplantation
As regulatory T cells are essential for the induction and preservation of peripheral tolerance and hence for preventing graft rejection, they have been deeply studied and seriously taken into consideration as a new therapeutic tool. Data suggest that Tregs could exert a tolerant state to alloantigens in vivo by inducing a regulatory profile in alloreactive T cells. Before describing the therapeutic approaches by which we could take profit of Tregs, it is convenient to describe briefly the main steps where Tregs get involved suppressing allorejection to understand the multiple pathways that could be affected by manipulating these cells.
In the setting of any solid organ transplantation, donor APCs migrate to the lymph nodes and present allogeneic class I or class II MHC molecules to the recipient’s CD8+ and CD4+ T cells, respectively (direct presentation). Host dendritic cells can also display and present graft alloantigens to T lymphocytes (indirect presentation) resulting in naive T cells differentiation and proliferation into effector helper T cells and cytotoxic T lymphocytes. These effector T cells migrate back into the graft and mediate cellular rejection. The usefulness of Tregs resides in their capability of regulating this rejection process in different ways.
Tregs are able to induce cytotoxic T lymphocyte apoptosis via engagement of CTLA-4 (cytotoxic T lymphocyte antigen-4) and PD1 (Programmed cell death 1), granzyme A/B, TNF related apoptosis-inducing ligand (TRAIL), FAS/FAS-ligand pathway, the galectin/TIM-3 pathway and through IL-2 deprivation. On the other hand, Treg’s CTLA-4 binds with CD80/86 on APCs leading to the induction of indolamine-2,3-dioxygenase (IDO)[23,24] and LAG-3 binds with MHC-II preventing APC’s ability to activate effector T cells[25]. Other mechanisms mediated by Tregs as TGF-β membrane-bound active expression, upregulation of ICER (inducible cAMP early repressor)[26] and the consequent inhibition of NFAT and IL-2 transcription by cAMP transference from Tregs to effector T cells, IL-10/IL-35/TGF-β production and miRNA exosome[27] transference are also suppressive physiological cues focused on diminishing immune response and rejection.
3. - T-immunotherapies (from Tregs to CARTregs)
Diverse therapies based on the use of immune-related cells to induce tolerance are currently undergoing clinical trials. Tolerance induction could be advantageous in different circumstances such as autoimmunity, in which control of self-reactive lymphocytes is defective, or transplantation. Even though Tregs are the cornerstone of this review, other cell strains are being considered and studied as tolerance inductors like myeloid-derived suppressor cells (MSDC), Mesenchymal Stem Cells (MSC), regulatory macrophages (Mreg), tolerogenic Dendritic Cells (Tol-DCs) or regulatory B lymphocytes (Breg).
3.1. Polyclonal Treg cells
Polyclonal Treg cells are non-antigen-specific cells (in contrast with antigen-specific Tregs we will describe later). Regulatory T cells are a well-defined subset that can be cultivated and expanded ex vivo and returned safely to patients. The low rate of Tregs in adults (less than 9% of CD4+) requires their expansion ex vivo before clinical use. Polyclonal expansion generates large numbers of Tregs from peripheral blood with potential use as adoptive cell therapy. First of all, cells can be sourced directly from the patient (autologous) or a third-party unrelated donor (allogeneic). The source of autologous Treg cells is limiting and current manufacturing conditions are demanding and costly. On the other hand, allogeneic Tregs offer exceptional opportunities when immune host-mediated elimination of transferred cells is overcome, allowing a durable response.
In terms of production and isolation, the best marker to characterize Treg cells is a nuclear transcription factor (FOXP3) and therefore is not suitable for isolation by flow cytometry since it is an intracellular complex. As described above, CD25 is highly expressed in most Treg cells but is transiently shared with effector T cells, so cannot be used by itself to avoid unwanted T-cells [28].
In the present day, there are different protocols for regulatory Treg production. One option is to use CD8, CD14, CD19 and CD127 negative selection to discard non-CD4 T-cells followed by CD25 positive selection[28]. Instead of selection, Treg induction protocol is based on FOXP3 expression promoters (IL-2, TGF-β activation and use of mTOR inhibitors). By using mentioned promoters together with TCR activation we could selectively stimulate Treg development[28]. Once we have selected/induced Treg subset, expansion and proliferation is required; IL-2 is used as a growth factor promoting expansion and survival of Tregs previously isolated [29].
Clinical trials to determine the safety and stability of this cell therapy have been carried out. In solid organ transplantation, the ONE study (NCT02129881) has shown that Treg cells can be grown and are safe for administration to transplant recipients in a dose-escalating approach from 0.5-3.0x106 cells/kg. There is an attractive argument for combining Treg with rapamycin (RAPA) monotherapy, since rapamycin may facilitate the survival of Tregs. Starting from ONE study, the so-called TWO study (MR/N027930/1), which started in 2017 and will end in 2023, aims to elucidate if nTreg can actually control rejection. For this purpose, 34 renal transplant recipients will be recruited over three years and each receptor will be treated with conventional immunosuppressive drugs. However, after transplant, cellular therapy of Treg isolated from their own blood (autologous) will be administered. Then, the immunosuppressive drug dose will be reduced while renal function monitoring is carried out. Thus, evidence of nTreg role in protecting grafts from damage could be tested[30].
3.2 Antigen-specific Treg therapies
Efficacy of antigen-specific Tregs should be higher than polyclonal Tregs [31,32] but their expansion is challenging due to low precursor rates. Some studies suggest that these alloantigen-expanded Tregs are 100-fold more potent at suppressing alloantigen-stimulated proliferation in vitro than polyclonal Tregs [33]. Different approaches to obtain antigen-specific Tregs should be taken into account: 1) purified antigen-specific Tregs; 2) specific TCR transduction; 3) CAR Tregs, in which the CAR (Chimeric Antigen Receptor) recognizes specific targets; and 4) specific effector T cells reconverted into Treg cells by FOXP3 overexpression.
1. Purified antigen-specific Tregs
The frequency of direct allo-reactive Tregs (darTregs) has been estimated to be between 1% and 10% [33]. Proof-of-principle researches have shown that antigen-specific Tregs can be cultured and expanded using donor APCs such as DCs, B lymphocytes[34] and mononuclear cells. Qizhi et al[35] group estimated that 5 × 109 polyclonal Tregs would be necessary to induce tolerance when combined with 90
In summary, new cell immunotherapies are appearing as options for control rejection in transplantation; probably the use of Tregs seems to be most promising, although other similar cell therapies are arriving to boost this option. The promise of a durable tolerance without unwanted immuno suppression is now a clear possibility in the near future.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.
